In the course of normal life there is a continuous recycling process of building new materials and breaking down old ones ready for disposal. This activity takes place in a special part of the body’s cells called the lysosome. Molecules are also secreted into their surroundings to form a meshwork of macromolecules called the extracellular matrix. This process requires a series of biochemical tools called enzymes.
Normally the breakdown of various components of the extracellular matrix are carried out by the enzyme matrix metallopeptidase 14. This enzyme also switches on (activates) another enzyme called matrix metallopeptidase 2. Matrix metallopeptidase 2 is important for a variety of body functions, including bone remodelling, a normal process in which old bone is broken down and new bone is created to replace it.
In people with Winchester syndrome, matrix metallopeptidase 14 is not produced or does not function normally which results in the build-up various components of the extracellular matrix and a reduction of matrix metallopeptidase 2. When there is not enough matrix metallopeptidase 2 signs and symptoms of Winchester syndrome begin. Initially babies may show little sign of the disease but it becomes more apparent as more and more symptoms start to appear as they grow.
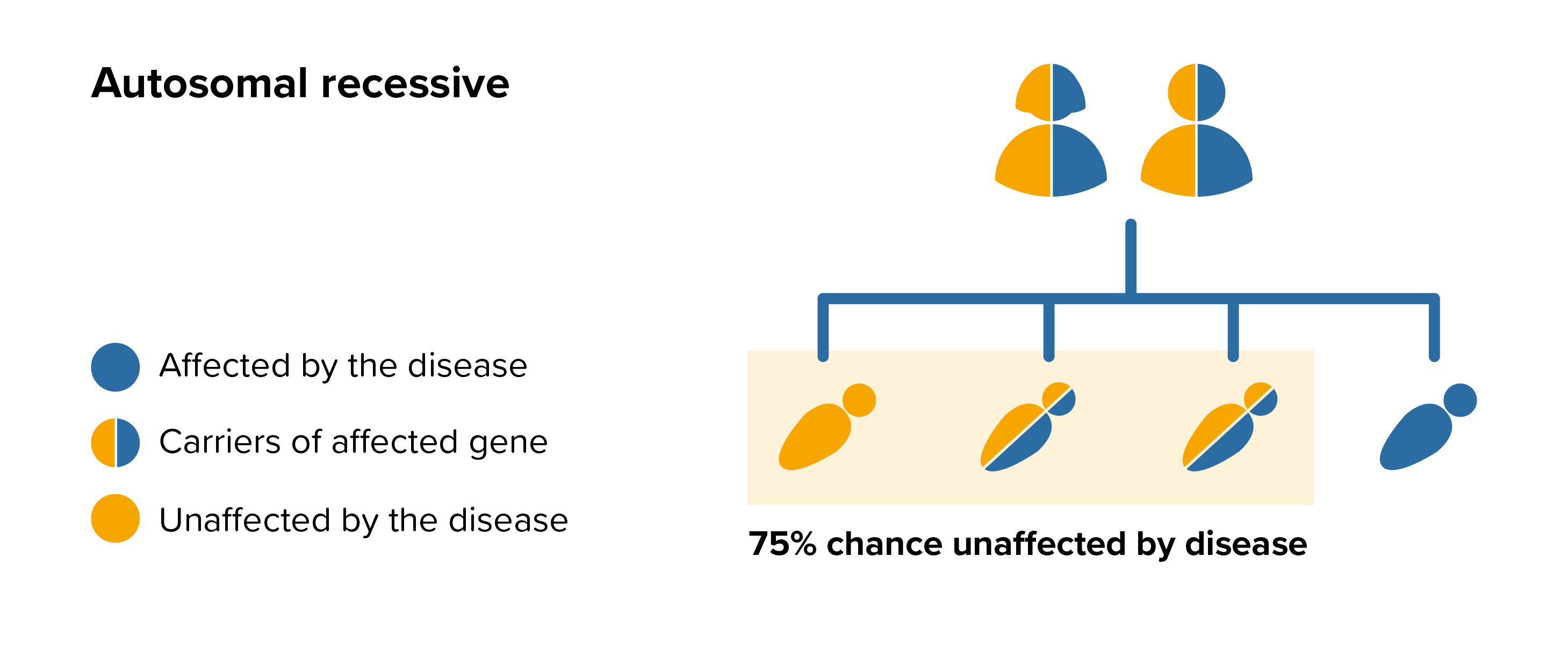 All parents of children with Winchester syndrome can benefit from genetic counselling, the counsellor can provide advice on the risk to close relatives and to suggest whether the wider family should be informed. To find out during a pregnancy, if the baby is affected by Winchester syndrome, screening tests can be arranged early on during a pregnancy for those families who already have a child with Winchester syndrome.
All parents of children with Winchester syndrome can benefit from genetic counselling, the counsellor can provide advice on the risk to close relatives and to suggest whether the wider family should be informed. To find out during a pregnancy, if the baby is affected by Winchester syndrome, screening tests can be arranged early on during a pregnancy for those families who already have a child with Winchester syndrome.