In the course of normal life there is a continuous recycling process of building new materials and breaking down old ones ready for disposal. This activity takes place in a special part of the body’s cells called the lysosome. This process requires a series of biochemical tools called enzymes. Normally fats and proteins are broken down and they produce a molecule called free sialic acid. Free sialic acid is moved out of the lysosome by an enzyme called sialin. In people with SASDs sialin is not produced or does not function normally which results in the build-up of free sialic acid in the lysosomes. The build-up causes the specific signs and symptoms of free SASDs. Babies may show little sign of the disease, but symptoms start to appear as more and more cells become damaged by the accumulation of free sialic acid.
SASDs have been classified into three major types based on severity of symptoms. Symptoms can vary greatly but all forms share features of brain related impairment.
Infantile free sialic acid storage disease (ISSD) is the most severe
Intermediate Salla disease, severity of the disease is on a spectrum between ISSD and Salla disease
Salla disease is the mildest form.
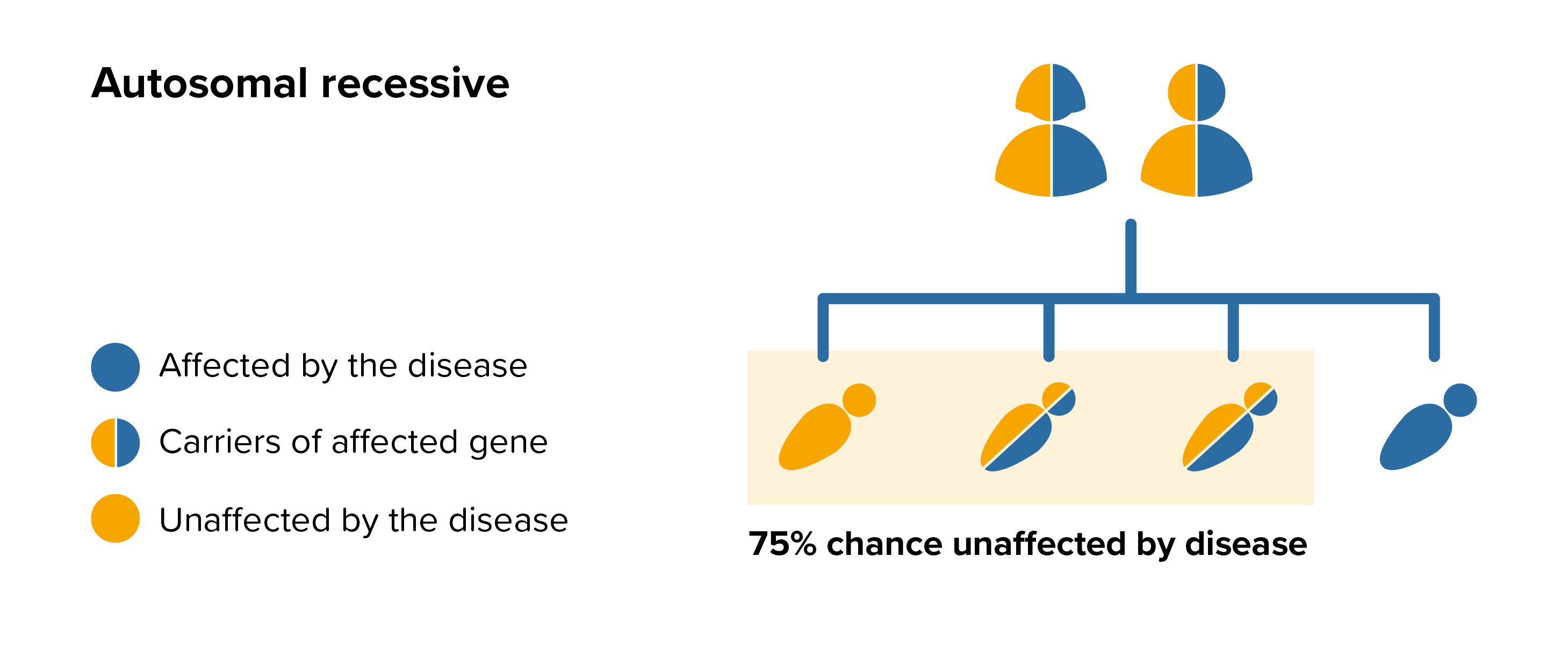 All parents of children with SASDs can benefit from genetic counselling, the counsellor can provide advice on the risk to close relatives and to suggest whether the wider family should be informed. To find out during a pregnancy, if the baby is affected by SASDs, screening tests can be arranged early on during a pregnancy for those families who already have a child with SASDs. Where only one parent is a carrier, they can opt for carrier screening but it is not 100% reliable or accurate and is not possible in all cases.
All parents of children with SASDs can benefit from genetic counselling, the counsellor can provide advice on the risk to close relatives and to suggest whether the wider family should be informed. To find out during a pregnancy, if the baby is affected by SASDs, screening tests can be arranged early on during a pregnancy for those families who already have a child with SASDs. Where only one parent is a carrier, they can opt for carrier screening but it is not 100% reliable or accurate and is not possible in all cases.