There is wide variation in the signs, symptoms and severity of MSD and not all the features will occur in everybody. MSD mainly affects the brain, skin, and skeleton. In the brain, deterioration of nervous tissue causes abnormal development (leukodystrophy). This leads to movement problems, seizures, developmental delay and slow growth. Life expectancy is shortened in those affected with all types of MSD. Typically, people with MSD survive only a few years after the signs and symptoms appear, but life expectancy varies depending on the severity and how quickly the brain related problems worsen.
MSD has been classified into three types based on severity of symptoms. Symptoms can vary greatly but all forms share features of brain related impairment:
neonatal is the most severe
late-infantile type is the most common
juvenile type is the rarest.
Neonatal MSD
Signs and symptoms appear soon after birth. Infants have deterioration of tissue in the nervous system, which can contribute to movement problems, seizures, developmental delay, and slow growth. They also have dry, scaly skin (ichthyosis) and excess hair growth (hypertrichosis). Skeletal abnormalities can include abnormal side-to-side curvature of the spine (scoliosis), joint stiffness, and other skeletal abnormalities. Infants with the neonatal type typically have facial features that can be described as coarse, may also have hearing loss, heart malformations, and an enlarged liver and spleen. Many of the signs and symptoms of neonatal MSD worsen over time.
Late-infantile MSD
This is the most common form of MSD. It is characterised by normal development in early childhood followed by a progressive loss of intellectual abilities and movement due to leukodystrophy or other brain abnormalities. Children with this form do not have as many features as those with the neonatal type, but they often have scaly skin, skeletal abnormalities, and coarse facial features.
Juvenile MSD
The rarest form of MSD, signs and symptoms of the juvenile type appear in mid to late childhood. Affected children have normal early development but then experience a slowing down of intellectual abilties and a reduction of physical movements. The regression in the juvenile type usually occurs at a slower rate than in the late-infantile type. Scaly skin is also common in the juvenile type of MSD.
Appearance
Growth is usually significantly restricted in people with MSD but this depends on the severity of the disease. People with MSD tend to bare a close resemblance to each other with many similar features. They may have large heads, low set ears and a flat bridge of the nose. The lips may be thickened and the tongue enlarged. As the disease progresses, the facial features become coarser.
Brain
Some affected children have experienced severe development delay from infancy. Children with MSD usually attain the ability to pull themselves up to a standing position and have relatively normal early language skills. However, children affected with MSD will gradually lose the skills they have learnt including being able to sit, stand and speak.
A number of children who are severely affected by MSD will develop epilepsy. There are different forms of epilepsy e.g. absence episodes where the child may appear to be staring into space with or without jerking or twitching movements of the eye muscles, or more generalised tonic-clonic seizures, a type of generalised seizure that affects the entire brain. Tonic-clonic seizures are more commonly associated with epilepsy. Most children will respond well to anticonvulsant medication.
Heart
Heart disease is common in children with the severe form of MSD but may not cause major problems. Some children with the less severe form of MSD may develop problems with one of the heart valves. The heart valves can be weakened and can fail to close tightly enough allowing small amounts of blood to leak back again. Problems with the valves can lead to valvular heart disease and if the condition worsens an operation may be needed to replace the damaged valves. An electrocardiogram (ECG) test is used to identify problems with heart muscle, function and valves, it is a painless procedure and is often carried out annually (or as often as the doctor thinks necessary) to show whether any problems are starting.
Lungs
Normally the ribs are curved and between the ribcage and breastbone there is flexibility for the chest to move freely. In MSD the chest cannot move freely to allow the lungs to take in a large volume of air because there is limited flexibility between the ribcage and breastbone. The muscles at the base of the chest may be pushed upwards by an enlarged liver and spleen, further reducing the space for the lungs. Additionally, the tissue of the lungs becomes thickened by stored mucopolysaccharides and stiffer than usual. When the lungs are not fully cleared there is an increased risk of infection which can lead to scarring causing further obstruction.
Typically, the bridge of the nose is flattened and the passage behind the nose is smaller than usual due to poor growth of the bones in the mid-face. The combination of abnormal bones and storage of mucopolysaccharides in the soft tissues in the nose and throat can cause the nose to become easily blocked. Frequent coughs, colds and throat infections are common problems for many people with MSD. Removal of tonsils and adenoids may help in some cases to lessen the obstruction and make breathing easier, but adenoid tissue may grow back. The neck may be short and this may contribute to the problems in breathing. The windpipe (trachea) becomes narrowed by storage material and is often more floppy, or softer than usual, due to abnormal cartilage rings in the trachea. Nodules or excess hardening of tissue can further block the airway.
Medication for controlling cough and cold symptoms and mucus production is available but it is essential to consult the doctor rather than using ‘over the counter’ medication which may not help. Medications such as antihistamines may dry out the mucus making it thicker and harder to dislodge. Decongestants usually contain stimulants that can raise blood pressure and narrow blood vessels, both are undesirable effects for people with MSD. Cough medicines that have a sedating effect may cause more problems with sleep apnoea by depressing muscle tone and respiration. It is common for people with MSD to develop secondary bacterial infections which should be treated with antibiotics.
Liver, Spleen and Abdomen
In most people with MSD the liver and spleen become enlarged by storage of mucopolysaccharides (hepatosplenomegaly), this often makes the tummy area bigger.
Bones and joints
Joint stiffness does lead to limited movement, in the shoulders and arms, hips and knees. The limited movement can make everyday activities like getting dressed difficult. Joint stiffness can sometimes cause pain which may be relieved by warmth and painkillers, speak with your doctor to select the most suitable treatment.
The shape of the hands is very noticeable, they are short and broad with stubby fingers which gradually become curved over or clawed. People with MSD sometimes experience pain, weakness or loss of feeling in the fingertips, this is caused by thickening of the ligaments which causes pressure on the nerves. It is called carpal tunnel syndrome and can be relieved by an operation. An electrical test called a nerve conduction study can show whether carpal tunnel syndrome is the cause.
Ears
Some degree of deafness is common in people with MSD. It may be conductive deafness, nerve deafness or both (called mixed deafness) and can be made worse by frequent ear infections.
Conductive deafness is when sound waves that travel through the ear canal, drum and the middle ear are impaired. Correct functioning of the middle ear depends on the pressure behind the ear drum being the same as that in the outer ear canal and the atmosphere. This pressure is kept equal by the eustachian tube which runs from the middle ear to the back of the nose. If the eustachian tube is blocked the pressure behind the eardrum will drop and the transmission of sound waves will be impaired. If this persists, fluid from the lining of the middle ear will build up and in time will become thick like glue, hence the condition being known as glue ear. Glue ear can be treated through surgery by inserting a small ventilation tube called a grommet, however these can fall out quickly and T-tubes, a type of grommet which stays in place longer, are an alternative option.
Nerve deafness is damage to the tiny hair cells in the inner ear. It may happen at the same time as conductive deafness, in which case it is referred to as mixed deafness. Mixed deafness can be managed by grommets or hearing aids. Nerve deafness is managed by fitting hearing aids in most people. More severely affected children may keep pulling out their hearing aids at first, but it is important to persevere at wearing them so that communication can be maintained. Alternatives include radio aids and the loop system which can be helpful at school and at home.
Eyes
People with MSD can experience clouding of the cornea which is caused by stored mucopolysaccharides and can lead to significant visual disability. Some people cannot tolerate bright lights as the clouding causes bending of the light which affects the vision, tinted glasses may be helpful in such circumstances. Severe corneal clouding may reduce sight, especially in dim light, a loss of night vision is common.
Dental
Good dental hygiene is very important for children with MSD, teeth should be well cared for to avoid tooth decay, pain and extractions. Usually teeth are widely spaced and poorly formed with fragile enamel. Cleaning around the mouth with a small sponge or a stick soaked in mouthwash will help keep the mouth fresh and avoid bad breath. If the water in your area has not been treated with fluoride, speak with your dentist about including fluoride tablets or drops as part of the dental management plan. Dribbling is a common problem and can soak through clothes causing soreness, to prevent this choosing a bib that is plastic backed.
It may be safer for any treatment to be carried out in hospital. If teeth need to be removed under anaesthetic this should be carried out in hospital under the care of an experienced anaesthetist and never in the dental surgery. It is important to inform the dentist about heart problems when discussing any treatment. This is because certain bacteria in the mouth may get into the blood stream and cause an infection on the heart valves. In most cases antibiotics are usually prescribed before and after any dental treatment.
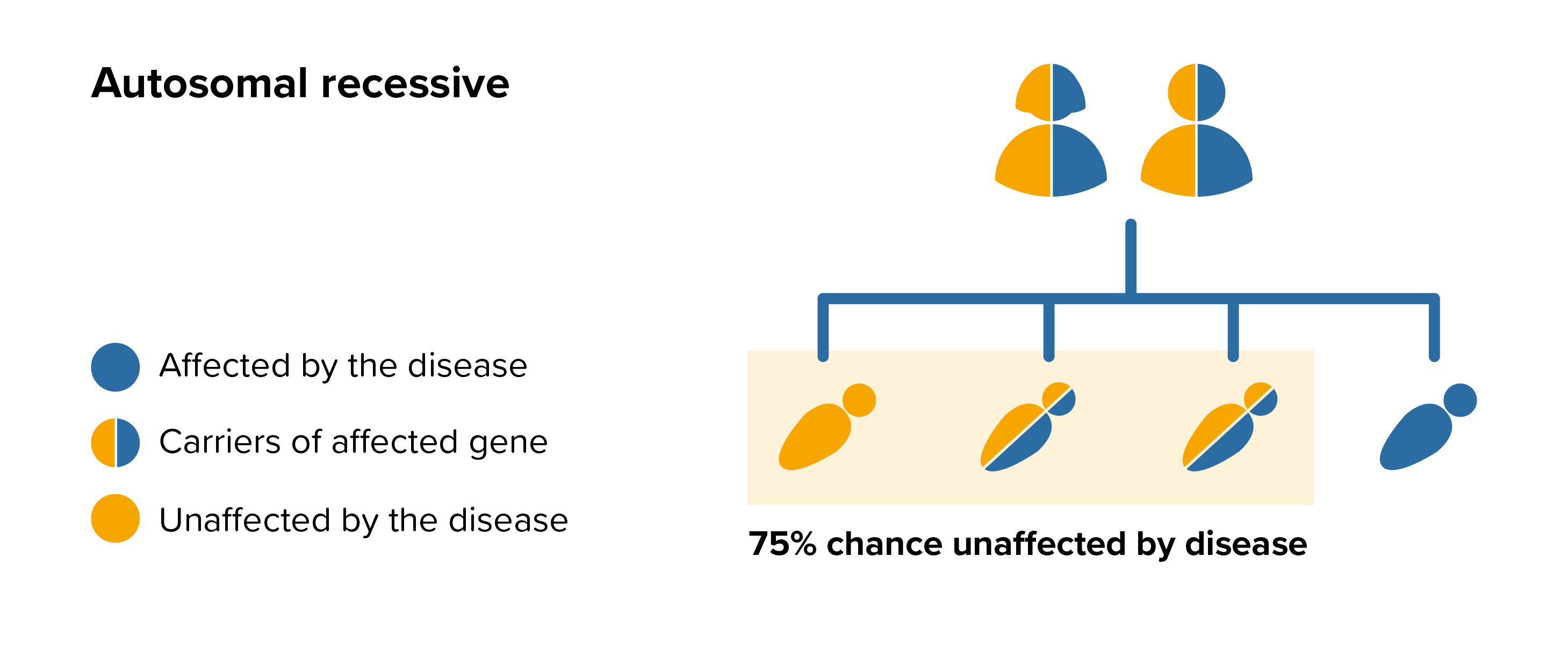 All parents of children with MSD can benefit from genetic counselling, the counsellor can provide advice on the risk to close relatives and to suggest whether the wider family should be informed. To find out during a pregnancy, if the baby is affected by MSD, screening tests can be arranged early on during a pregnancy for those families who already have a child with MSD. Where only one parent is a carrier, they can opt for carrier screening but it is not 100% reliable or accurate and is not possible in all cases.
All parents of children with MSD can benefit from genetic counselling, the counsellor can provide advice on the risk to close relatives and to suggest whether the wider family should be informed. To find out during a pregnancy, if the baby is affected by MSD, screening tests can be arranged early on during a pregnancy for those families who already have a child with MSD. Where only one parent is a carrier, they can opt for carrier screening but it is not 100% reliable or accurate and is not possible in all cases.